
“TL;DR: Cellulite, a condition shrouded in misinformation, plagues the media with myths such as “cellulite is toxins” or “dry brushing reduces it.” Far from being mere fat or a fabricated issue, cellulite stems from complex anatomical and physiological changes in the skin’s deeper layers. Quality research—via ultrasound, MRI, and biochemistry—reveals it as enlarged adipose tissue compartments in the dermis and hypodermis, coupled with lax skin, inflammation, water retention, and fibrotic collagen bands. These “fat pouches” push upwards while shortened “collagen strands” pull downwards, creating the familiar mattress-like appearance—think cottage cheese or orange peel. Scientifically, cellulite is best termed “Oedematous FibroSclerotic DermoPannicullopathy” (OFSDP), encapsulating its hallmarks: oedema, fibrosis, and inflammation. A more comprehensive label, “Toxic Flaccid Oedematous FibroSclerotic DermoPanniculitis” (TFOFSDP), acknowledges toxin accumulation and skin laxity, though its length may deter adoption. Cellulite’s complexity—a vicious cycle of fat expansion, connective tissue damage, and poor circulation—renders most treatments ineffective. Only a multifaceted approach targeting all aspects can yield meaningful reduction. Advanced treatments such as high-power radiofrequency and ultrasound cavitation target fat and fibrosis, while creams with potent actives like caffeine and forskolin address inflammation and circulation. Coupled with a healthy diet and vigorous exercise, this multifaceted approach tackles all aspects of cellulite, delivering significant, lasting results where simplistic solutions fail.”
Cellulite: all you needed to know
Cellulite: what it is exactly, what causes it and how it is formed
Cellulite: anatomy & physiology
Scientific cellulite definition I
Scientific cellulite definition II
Cellulite explained
Cellulite diagram image
Cellulite ultrasound image
Cellulite, connective tissue and adipose tissue
Fat pouch peaks and collagen strand troughs
Cellulite anatomy: the cellulite mattress appearance
Cellulite’s downward spiral
Cellulite physiology: a web of complications - literally and metaphorically
The vicious circle of cellulite must be broken at multiple points, if we want to make some real progress with cellulite reduction
To reduce cellulite a comprehensive approach is needed
Have a skin tightening/cellulite treatment in London with the cellulite experts
Advanced, infrared / blue / red light therapy treatments in London at LipoTherapeia
The Cellulite School™: Get advanced training in cellulite reduction and skin tightening
Cellulite: what it is exactly, what causes it and how it is formed
There is ridiculous amount of misinformation on cellulite in the media.
Instagram, blogs, tiktok, youtube, newspapers, glossy magazines, clinics, salons, cellulite equipment manufacturers and cellulite cream manufacturers offer such wonderful gems as “cellulite is toxins”, “cellulite is just fat”, “cellulite does not exist”, “cellulite is natural”, “cellulite is normal”, “cellulite is just fascia”, “dry brushing reduces cellulite“, “lymphatic massage gets rid of cellulite”, “cellulite is just water retention”, “90% of women in the world have cellulite” etc etc.
For the vast majority of people, the perceived wisdom on the nature of cellulite is based on urban myths such as the above and is a mixture of confusion, ignorance, half-knowledge and misinformation.
With so much misinformation around cellulite, it is no wonder why most cellulite treatments are so ineffective: we cannot correct a problem if we are ignorant or misinformed about the problem’s nature.
And with so much confusion, one would think that there exists no research on the nature (anatomy and physiology) of cellulite and that it is all made up stuff. However, this could not be further from the truth.
There is plenty of quality research on the anatomy and physiology of cellulite and its causes, based on ultrasound, MRI, microscopy and biochemistry investigations, and this and two more of our articles (“Pre-cellulite: the origins of cellulite” and “Is cellulite normal?”) are all about presenting those facts.
Furthermore, this entire website is dedicated to providing information on cellulite and its treatment.
On this article you can read an accurate description - and view an accurate depiction - of cellulite, its causes and its formation, away from all the misinformation found on the web, social media and even most specialist books.
Cellulite: anatomy & physiology
Cellulite is enlargement of adipose tissue compartments at the dermis and hypodermis level, i.e. the medium and deep skin layers, respectively.
This adipose tissue compartment enlargement is almost always accompanied by:
Laxity at the dermis level
Inflammation and oedema (water retention) at the hypodermis level
Shortening and fibrosis of the retinaculae cutis (aka skin ligaments or “collagen bands”)
In cellulite:
Abnormally enlarged ‘fat pouches” push skin upwards
At the same time abnormally short and hard ‘collagen bands’ anchor the skin surface down to the deeper tissues more strongly than normal.
The combination of one upward force (‘fat pouches’) and one downward force (‘collagen bands’) makes fat pouches protrude upwards of the anchor skin around them. This results in the familiar mattress appearance of cellulite, also described as cottage cheese or orange peel skin (peau d ‘orange).
Scientific cellulite definition I
The best scientific definition of cellulite which describes it (almost) accurately is: "Oedematous FibroSclerotic DermoPannicullopathy (OFSDP)". This in plain English translates as: inflammation of the skin’s fat deposits, accompanied by scar tissue and inflammation / water retention.
The above includes all the hallmarks of cellulite in one elegant, four-word definition:
OEDEMA (water retention)
FIBROSIS-SCLEROSIS (scar tissue / hardening of connective tissue)
SKIN FAT (dermo-pannicullus)
INFLAMMATION (-opathy)
As SKIN LAXITY is found in 90% of cellulite cases, we should add the word “flaccid”, in which case we have: Flaccid Oedematous FibroSclerotic DermoPannicullopathy (FOFSDP).
We could perhaps also add the word toxic to the above definition, as the creation of cellulite is significantly accelerated by the accumulation of fat soluble toxins in adipose tissue.
So a revised, all-inclusive definition of cellulite could be: "Toxic Flaccid Oedematous FibroSclerotic DermoPanniculitis" (TFOFSDP).
But then the name becomes too long - plus the acronym is not that pretty, so I don’t expect it to catch any time soon - although it is very accurate and descriptive…
Scientific cellulite definition II
Another scientific definition of cellulite is: “DermoPanniculosis Deformans”. This basically means:
Inflammation of the skin’s fat tissue (dermopanniculosis)
Accompanied by deformity / fibrosis (deformans)
Not very comprehensive and still too much Latin…
Cellulite explained
To start explaining how cellulite develops, it is worth noting that fat in the deeper layers of the skin is always enclosed in little compartments wrapped up by a thin sheath of connective tissue, forming "fat pouches".
(Connective tissue is tissue made of a network of collagen, elastin and other proteins. Connective tissue is what keeps everything together and gives shape to our body.)
These fat pouches are literally suspended by collagen strands (retinaculae, skin ligaments, often erroneously called ‘septae’ or simply ‘septa’) that attach them:
To the surface of the skin above (dermis)
And to deeper tissues underneath (intermediate fascia)
This forms a three-dimensional suspension structure whose ‘tensegrity’ makes skin soft, but also firm and elastic at the same time.
These long, thick collagen strands (retinaculae) that run from the dermis above all the way to the intermediate fascia below are - together with the enlarged fat pouches - responsible for the mattress cellulite appearance.
Cellulite diagram
Here is a simplified (and somewhat inaccurate) diagram of cellulite
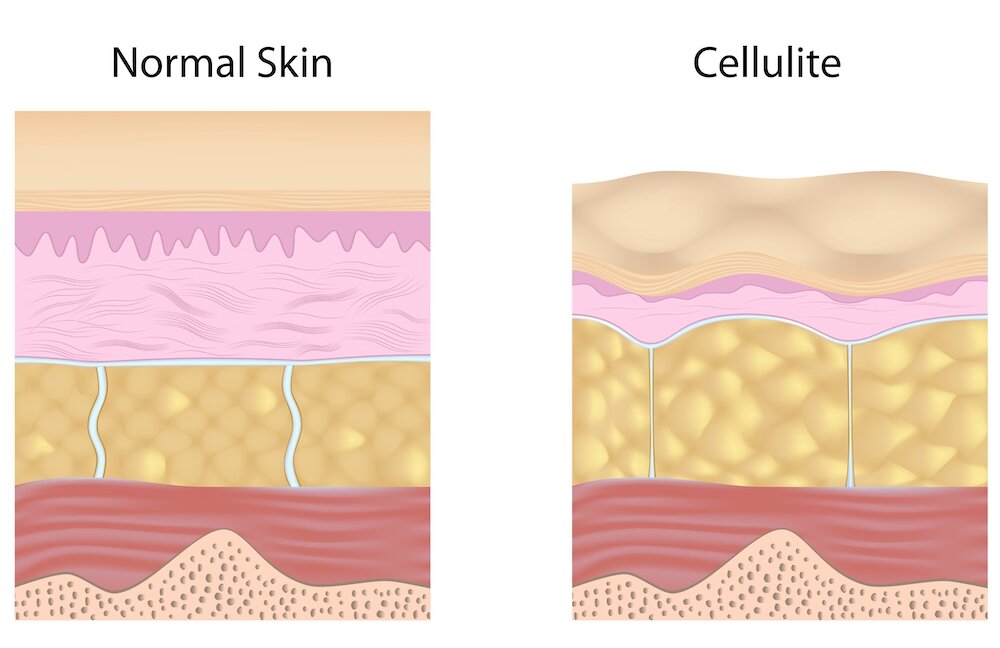
Simplified cellulite diagram, where the entire subcutaneous adipose tissue is missing. But it gives the general gist of it.
Cellulite ultrasound image
Here is a much more accurate depiction of cellulite with skin ultrasonography (our picture), so we know exactly what we are talking about

On top you can see the epidermis in light grey/white
Below it is the dermis in grey
Below that you can see the hypodermis with a cellulite globule circled and with white/grey retinaculae left and right of it. Fat is depicted in dark grey / black here.
Below that you can see the intermediate fascia in quite bright white
Below that is the subcutaneous adipose tissue, depicted in dark grey / black here and with the occasional retinaculae and fascial planes in light grey / white
Further down you can see two layers of deep fascia in light grey / white
Below that would be the muscles of that specific area (very little shown, mainly on the left)
Cellulite, connective tissue and adipose tissue
Connective tissue refers to collagen and elastin rich tissue that gives shape to our body and keeps it together: ligaments, tendons, fascia, sheaths, skin ligaments/retinaculae, skin/dermis and it is also a constituent of muscles, bones, blood vessels and organs.
As such, connective tissue is an important aspect of cellulite.
What most people do not know, however, is that adipose tissue is a subtype of connective tissue, which is rich in fat. And adipose tissue is the most important aspect of cellulite.
As adipose tissue forms part of connective, we can say the cellulite is a connective tissue aesthetic condition.
Fat pouch peaks and collagen strand troughs
Now, it is also worth noting that fat cells can swell up to 3,000 times their normal volume.
As these fat pockets enlarge with excess fat and water, they expand and push the skin surface upwards
On the other hand, in reaction to the pushing of fat outwards, the collagen strands that connect the surface of the skin above to the deeper tissues below, become overstretched and injured
This injury eventually leads to scarring, shortening and hardening (fibrosis) of the collagen strands, eventually culminating in the skin being pulled downwards at those points
Cellulite anatomy: the cellulite mattress appearance
The peaks (caused by fat pushing the skin out) and troughs (caused by skin ligaments pulling the skin down) cause the mattress appearance that we call cellulite.
If dermis (the main skin layer) is loose, it allows itself to be deformed more easily, and the mattress appearance becomes more pronounced.
In this picture:
• The sofa’s upholstery foam corresponds to fat
• The upholstery leather corresponds to the weakened dermis, the skin’s main layer
• The upholstery button threads correspond to the collagen strands / skin ligaments / retinaculae
Cellulite’s downward spiral
There are hundreds of anti-cellulite creams around but 90% of those creams don't really work
90% of beauty salons offer some sort of cellulite treatment
And 90% of those treatments fail to offer you anything more than a slight, temporary reduction of cellulite
And the obvious question is: why?
The answer to the "Why” question is the multi-faceted nature of cellulite.
In one small area of skin you can have connective tissue hardening (fibrotic retinaculae) yet at almost the same spot you also have skin looseness (lax dermis); AND water retention; AND inflammation; AND excessive fat accumulation.
And each of those things reinforce the other, in a perpetual vicious circle that gradually destroys the very fabric of the skin in the legs, buttocks and - quite often - stomach, waist and arms.
An analysis of this vicious circle follows.
Cellulite physiology: a web of complications - literally and metaphorically
Remember how we described cellulite earlier as a three-dimensional web structure? Well, that was referring to a literal, physical web. However, the problem with cellulite is also another, metaphorical web: the web of complications.
Cellulite is characterised by a web of reinforcing feedback mechanisms:
Inflammation, as any biology student knows, leads to water retention and vice versa, in a perpetuating negative loop
Inflammation quite often leads to fibrosis / sclerosis (scar tissue / tissue hardening)
Water retention inhibits fat removal, but does not prevent fat accumulation ("fat trap" effect)
An excess of adenosine and alpha2 adrenoreceptors in the fat tissue, due to chronic exposure to oestrogen, also inhibits fat removal, but does not prevent fat accumulation ("fat trap" effect)
Every month the menstrual cycle is accompanied by the release of MMPs (matrix metalloproteinases), which break down collagen, thereby weakening the dermis
Ever expanding fat tissue (due to excess calorie / sugar consumption) further injures the connective tissue strands attached to it and causing more fibrosis / sclerosis
On the other hand, ever expanding fat tissue breaks down the connective tissue around it, causing skin looseness. Ever wondered why fat makes your skin flabby? That's why, fat eats into your skin.
Furthermore, ever expanding fat tissue mechanically inhibits circulation, causing more water retention
Water retention / poor circulation leads to adipose tissue hypoxia, which is well known to cause inflammation, oxidative damage, fibrosis and glycation (connective tissue protein damage due to sugar consumption). And vice versa - all reinforcing each other.
Toxins from food, alcohol, cigarettes/vaping, plastics/BPA/contraception accumulate in the fat tissue and cause further fat tissue inflammation, hypoxia and glycation
As you see, it just goes on and on and on.
One complication causes another, which causes another, which causes another, and the whole thing becomes a never ending vicious circle.
The vicious circle of cellulite must be broken at multiple points, if we want to make some real progress with cellulite reduction
Attempting to break this web at just one point, as in with a single ingredient cream or with a "fascia blasting massage" is naive, to say the least.
In addition reducing food intake is by itself not enough either, as evidence shows
And the same applies to "cellulite exercises" (hint: they don’t exist), as every woman knows
A bit of lymphatic drainage to (very temporarily) reduce water retention is clearly nowhere near enough
And let's not even talk about the pathetic joke of "dry skin brushing" 😂
Some caffeine cream to marginally boost fat removal and circulation will not do it either. Otherwise, with the amounts of coffee women drink today, there would be no such a thing as cellulite. Caffeine does help, but on its own is not even close enough to effectively remove cellulite.
And let's not even mention the sheer time-wasting ritual of rubbing ground coffee on thighs 😂
To reduce cellulite a comprehensive approach is needed
A good cellulite treatment should work on both skin laxity AND hypodermal fat reduction AND poor circulation AND fibrosis reduction:
The strongest, most effective, SAFE cellulite technologies currently are deep-acting, high-power radiofrequency and high-power ultrasound cavitation. high-power LED phototherapy, provided right after these technologies, enhance their effectiveness, for maximum results, naturally.
There is no known technology that directly works on the other aspects of cellulite, i.e. inflammation, oxidative damage or glycation, but there are plenty of natural topical active ingredients which help in that direction
And the same applies to creams: a good cellulite cream must contain actives which are well established to work against many, if not all aspects of cellulite: fat AND poor circulation AND oxidative damage AND glycation AND fibrosis AND inflammation AND skin laxity:
The best anti-cellulite cream is one one with multiple, high-purity anti-cellulite actives in high concentrations
Well-researched anti-cellulite actives include caffeine, asiatic acid, asiaticoside, madecassic acid, madecassoside, forskolin, EGCG, escin, esculin, chlorogenic acid, hydroxyproline, cocoa flavanols and curcumin, among others
Furthermore, both treatments and creams have to be combined with healthy eating; vigorous exercise (sorry, relaxing Yoga and Pilates classes don't count); and sugar / smoke / alcohol / BPA / contraceptive pill avoidance, if some good results are to be expected and maintained.
This is how cellulite is reduced: by attacking it on all seven fronts.
Have a skin tightening/cellulite treatment in London with the experts
At LipoTherapeia we have specialised 100% in skin tightening and cellulite reduction for more than two decades and 20,000+ sessions.
This is all we study and practise every day and have researched and tried hands-on all the important skin tightening equipment and their manufacturers.
As strong, deep acting radiofrequency and deep-acting, high-power ultrasound cavitation are the technologies of choice for skin tightening and cellulite reduction, we have invested in the best RF/ultrasound technologies in the world.
Furthermore, over the last two decades we have developed advanced RF and cavitation treatment protocols in order to make the most of our technologies, for maximum results, naturally and safely.
And for even better, faster results, we now combine our RF/ultrasound treatments with high-power red/infrared light LED treatment.
Our radiofrequency/ultrasound/LED treatments are comfortable, pain-free, downtime-free, injection-free, microneedling-free, 99.5%+ safe and always non-invasive.
And our focus is on honest, realistic, science-based treatment, combined with caring, professional service, with a smile.
We will be pleased to see you, assess your cellulite, skin laxity or fibrosis, listen to your story, discuss your case and offer you the best possible treatment.
Advanced, infrared / blue / red light therapy treatments in London at LipoTherapeia
At LipoTherapeia we are passionate about phototherapy (also known as photobiomodulation/PBM, red light therapy, infrared light therapy, blue light therapy, LED light therapy etc) and we use the most powerful equipment available today (up to 200mW/cm2), for best results and treatment of large body areas.
We use specialised therapy protocols for skin rejuvenation / anti-ageing, pigmentation / post-inflammatory hyperpigmentation (PIH), moderate/severe acne, skin redness, sensitive/inflamed/irritated skin, wound healing, sports injuries / musculoskeletal pain and overall wellness / well-being.
Our LED phototherapy sessions are comfortable, deeply relaxing and super-safe and are great to enhance our radiofrequency/ultrasound treatments for skin tightening / cellulite reduction.
On our booking page you can book stand-alone phototherapy sessions or combine them with our other treatments, as an add-on.
Learn more or check prices and book an expert LED phototherapy treatment at our London clinic.
The Cellulite School™: Get advanced training in cellulite reduction and skin tightening
Do you want to deeply understand radiofrequency, ultrasound cavitation, LED phototherapy, cellulite and skin tightening?
Attend a half-day, 1-day, 2-day or 3-day one-to-one masterclass and confidently offer your clients the safest, strongest and most effective treatment possible.
Service available via Zoom or at our central London practice.
Learn more or check prices and book training at our London clinic or via Zoom.